Super ultrasound helps doctors win the vein game




That misery is history when doctors make use of the latest ultrasound technology to scan for the best veins and help them guide their needles.
“We’ve moved from guesswork to science,” says Dr Elizabeth Prentice, specialist paediatric anaesthetist at Royal Children’s Hospital, Melbourne (RCH). “We have used ultrasound for several years for central venous access, but now even with peripheral venous access and arterial lines, once you’ve failed a few times at using surface anatomical landmarks and hoping the vein’s where it should be, you move to a scientific approach where you scan the patient with the ultrasound, choose the best vein, the best position, and you don’t have any attempts if there are no suitable veins there.”
You move to a scientific approach where you scan the patient with the ultrasound, choose the best vein, the best position..
Prentice is part of a team of vascular-access specialists among the more than 20 consultant anaesthetists at RCH. “All of the anaesthetists are using the ultrasound machines now,” she says. “The technology got much better about two years ago, but it’s even better with the new machines—we’re just amazed by how easy it is to see these tiny little veins and arteries. It’s made a huge difference to our practice.”
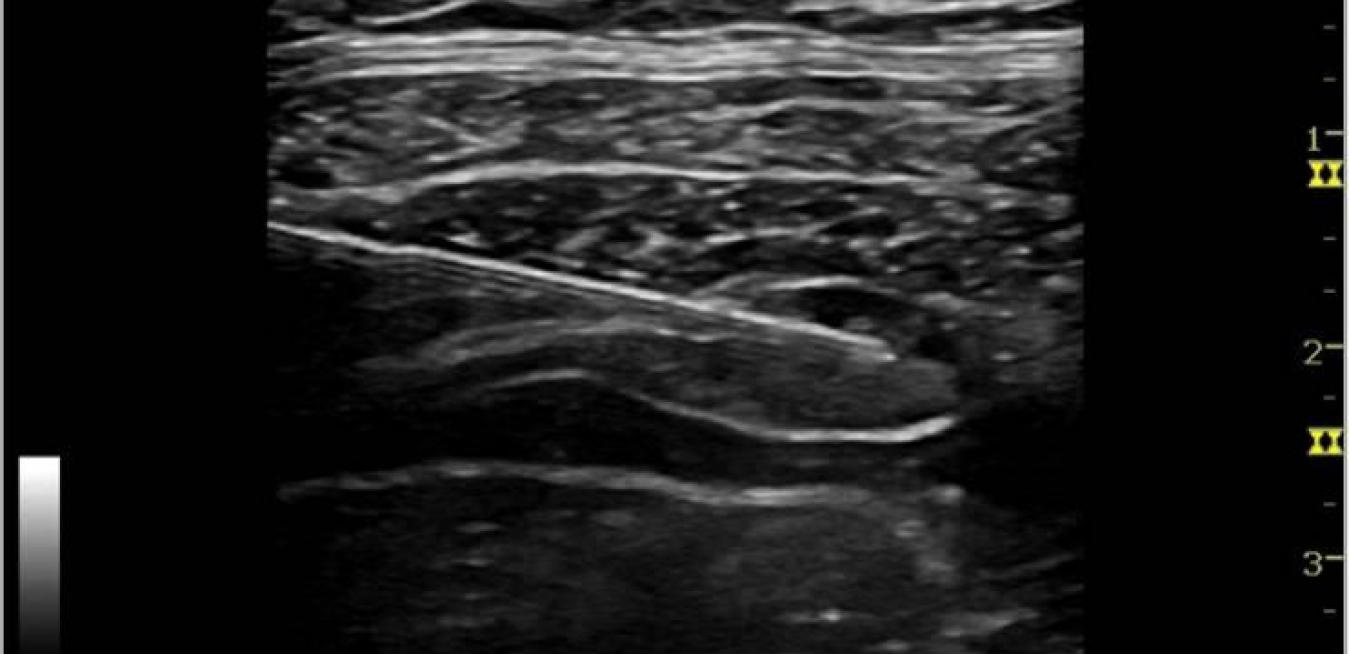
The new ultrasound machines at RCH—two of them—are GE’s LOGIQ e. “Specialists told us they need to see clearly, see quickly and guide precisely, and those needs drove the creation of the new LOGIQ e,” says Matt Tucker, general manager, ultrasound, GE Healthcare Australia and New Zealand. “In paediatric anaesthesia, the new high-resolution L10-22-RS transducer operates at frequencies of 22 MHz, which provides unprecedented image quality for resolving tiny vessels, aiding in precise guidance for cannulation.”
 veins preserved for life. The more attempts you have, or if you put the line in a vein that’s too little because you haven’t scanned, you risk those children not being able to have future PICCs—they have to get implanted vascular access ports. Ten years ago, cystic fibrosis kids might have had big PICC lines in tiny veins, because doctors weren’t able to assess them with ultrasound. Sometimes these kids’ arm veins were lost—the veins occlude and you can’t use them anymore. Today we would never do a PICC line or central line without an ultrasound.”
veins preserved for life. The more attempts you have, or if you put the line in a vein that’s too little because you haven’t scanned, you risk those children not being able to have future PICCs—they have to get implanted vascular access ports. Ten years ago, cystic fibrosis kids might have had big PICC lines in tiny veins, because doctors weren’t able to assess them with ultrasound. Sometimes these kids’ arm veins were lost—the veins occlude and you can’t use them anymore. Today we would never do a PICC line or central line without an ultrasound.”The stress reduction for patients, parents and doctors has been enormous. Prentice cites before and after quotes from parents of CF patients. One mother, of CF sufferer Harry, recalled a traumatic pre-ultrasound PICC line insertion: “A trainee doctor tried to put a line in and became very distressed. My son was hysterical and my husband and the nurses had to hold him down.” She contrasted this with Harry’s post-ultrasound world: “A pre-visit by an anaesthetist and an ultrasound machine got my son interested and involved—he loved seeing his muscles and his veins on the screen. The procedure itself went so smoothly and Harry said he didn’t feel a thing. It was over in about 15 minutes. I can’t adequately express how comparatively better this procedure was. It really is a game-changer for us.”